There are multiple modalities at one’s disposal to treat knee conditions

BY DR JONAS FERNANDEZ
I have lost count of the times patients have walked into the consultation rooms complaining that their knees hurt. They often attribute this condition to the lack of “lubricant” in the knee joints (the oft-used phrase is “kurang minyak”).
This pain they refer to is often due to osteoarthritis of the knee. The lubricant they refer to is the synovial fluid, a gel-like substance found naturally in the knee joint.
In simple terms, knee osteoarthritis is due to wear and tear (of the cartilage in particular). However, there are other causes of arthritis, like rheumatic diseases or the result of a knee injury.
From a molecular point of view, inflammatory processes play an essential role in the breakdown of these cartilages. There are multiple modalities at one’s disposal to treat this condition, ranging from medication and physiotherapy to injections and surgeries.
Injections
Let us zoom in on this particular treatment modality. Injections can be used to treat knee osteoarthritis and other types of orthopaedic conditions.
These conditions include shoulder impingement, De Quervain tenosynovitis, sciatica pain and many others. Different conditions often require a particular type of injection.
These include steroids, hyaluronic acid and/or processed blood products. Your doctor may prescribe the latter two in knee osteoarthritis, in isolation or in combination.
As an orthopaedic trainee at the University of Malaya, I had the privilege to work closely with some of the brightest minds in the Tissue Engineering Group at the National Orthopaedic Centre of Excellence for Research and Learning (NOCERAL).
Prof Dr Tunku Kamarul, Dr Chong Pan Pan and her team had developed a novel technique for treating osteoarthritis and other conditions using Platelet-derived Extracellular Vesicles (PEV).
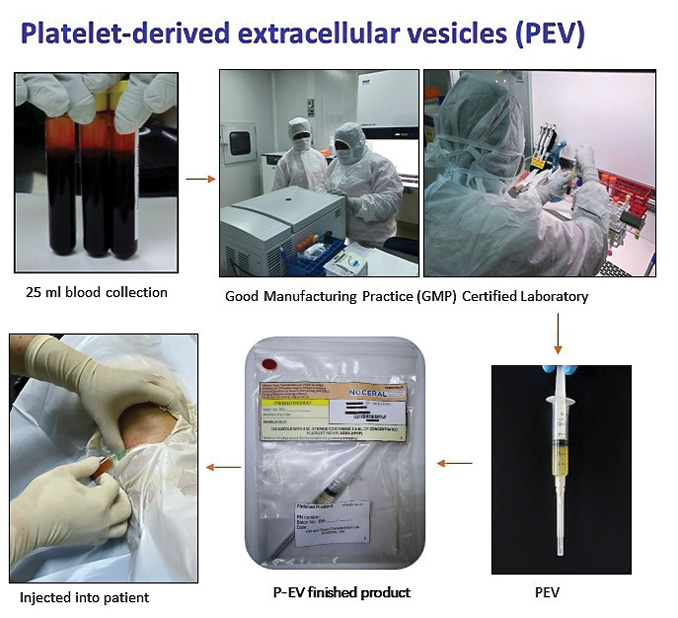
As part of my thesis as a Master’s student, I evaluated its efficacy in treating patients with knee osteoarthritis and compared it to Hyaluronic Acid (Hyruan ONE).
PEV is produced by first obtaining the patient’s blood and then processing it by spinning the blood. The product of this process is a fluid that is richly concentrated in these extracellular vesicles.
Many previous studies have demonstrated that PEV plays a role in stimulating cartilage regeneration, reducing inflammation, and playing a role in the homeostasis of the knee joint microenvironment.
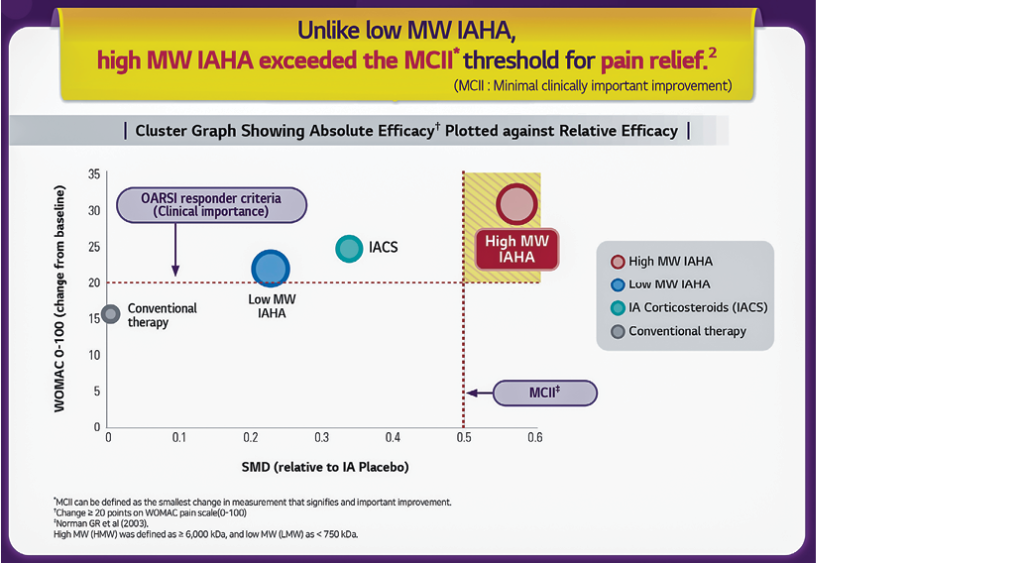
The other choice of injection, as mentioned earlier, is the Hyaluronic Acid (HA) injection. HA is a molecule seen naturally within the cartilage and synovial fluid.
They function by providing lubrication and shock absorption. As with the PEV, they have anti-inflammatory properties and help maintain knee homeostasis on a cellular level.
So do they really work?
There are many studies to suggest that intra-articular knee injection of either blood products or HA can reduce patients’ pain symptoms. In my thesis, this finding was no different.
We found that patients experienced lesser knee pain after the injection, which led them to be more mobile. As a result, they could go about their daily activities with minimal fuss, leading to healthier physical well-being and an improved emotional and mental one.
In combination with a local anaesthetic, a steroid injection is also often used in orthopaedic practice. Steroid plays a role in reducing inflammation, whereas the local anaesthetic helps alleviate pain symptoms.
Examples of their use include injections into the shoulder joint in cases of impingement syndrome, around the tendons and in some cases of spine diseases.
While all these injection options are meant to treat a patient’s symptoms, they don’t come
entirely risk-free. That said, each patients’ condition should be individualised and treated accordingly, as one shoe will not fit all. — The Health
Dr Jonas Fernandez is an Orthopaedic Surgeon at Putrajaya Hospital. He is also a member of the Malaysian Arthroscopy Society (MAS).







{kind=link}