
One can be suspected to have a knee injury based purely on history

BY DR JONAS FERNANDEZ
The knee is probably the most common joint injury suffered by athletes. Injuries can range from a simple bruise to complicated fractures and torn ligaments.
Many, if not all seasoned athletes, would have endured some injury in their careers. Surprisingly, these athletes can self-diagnose even before a single visit to the doctor.
I was no exception. During a national taekwondo tournament in 2004, I endured a ruptured Anterior Cruciate Ligament (ACL). Right after the injury, my friends and teammates were like, “this one surely ACL koyak (torn), bro”.
And they were right. Could you really diagnose someone with torn ligaments just like that? After all, this particular ligament is seated deep within the knee joint, so how could you say?
So the answer is Yes. You can suspect someone to have this injury based purely on history. With physical examination, one can be almost certain. Let’s start with the history first.
For this, allow me to take you down memory lane on my own torn ligament. Let me set the scene. As previously mentioned, it was a taekwondo tournament. There I was, in my first fight of the day, aiming to defend the national junior title I had won the year before.
Attempting to land a kick on my opponent, I turned my body, kicking with my right leg. My left foot was firmly planted on the ground during this kicking motion.
In one swift motion, I could feel my entire body turn as I twisted my knee. In short, my left leg was not in sync with the rest of my body’s motion, thus resulting in a twisting injury to the knee.
Swelling is almost immediate
There was an audible “pop” sound heard as this was happening. In agony, I fell to the ground, unable to stand up, let alone walk without assistance. As I rested, with ice on my knee, I had noticed that my knee had begun to swell up.
To summarise, the relevant history of the initial trauma includes the twisting mechanism injury, the pain, the “pop” sound, the inability to continue the sporting activity, and lastly, the almost immediate swelling.
After a couple of weeks of rest and icing the knee, the pain and swelling will slowly subside. One will slowly get back to walking in a few weeks and even back to some light sports.
Now that the pain and swelling have resolved, patients (and me at the time) will tend to get back into their sporting activities. This is when one might start to experience another symptom, instability.
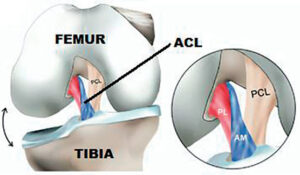
Before we get into that, some light anatomy class. The ACL consists of two bundles, namely the anteromedial (AM) and the posterolateral (PL).
The AM primarily controls the knee’s anterior translation, whereas the PM bundle holds the pivoting (twisting) motion.
Symptoms of instability can vary amongst patients. They usually present with the feeling of the knee “giving way” when walking on slippery or uneven ground, when ascending or descending the stairs and even when crossing over something (like a drain).
Apart from these symptoms, the athletes may complain of instability when making sudden pivoting movements. It includes motions like making sudden changes in direction, usually seen in court sports like futsal, basketball etc.
History-taking is critical
A thorough history-taking will usually reveal these symptoms and point the treating doctor in the right direction as physical examination starts. We’d look out for signs like swelling, bruising, tenderness and limitation in range of motion.

More specifically, one will need to perform particular tests like the Lachman Test, the Anterior Drawer Test to try, and the Pivot Shift Test to determine if the ACL is damaged.
With the history and examination, an ACL injury can be confidently diagnosed. However, it is imperative to remember other structures in the knee that may have been injured, too, like the meniscus and cartilages.
Finally, to confirm the diagnosis of an ACL injury and look out for other possible damages, your doctor might order a Magnetic Resonance Imaging (MRI) scan.
This scan allows us to visualise structures like the ligaments, meniscus and cartilages that we will not be able to see on an X-ray. Treatment begins with physiotherapy to ensure adequate muscle strength is retained and maintain a good range of motion.
Surgery is indicated if there is persistent instability, whereby your doctor might advise on the ACL reconstruction. However, it should be kept in mind that the success of the surgery is very much dependent on post-operative rehabilitation.
So, there you have it, go ahead and diagnose and treat that twisted knee of yours! — The Health
Dr Jonas Fernandez is an Orthopaedic Surgeon at Putrajaya Hospital. He is also a member of the Malaysian Arthroscopy Society (MAS).







{kind=link}